

Unusual does not equal disordered
Uncommon behavior is not automatically a disorder.
Resource Hub
A complete reference page for the psychology final project rubric: diagnosis, DSM changes, symptoms, prevalence, causes, treatment, lived experience, learning theory, and sources.
![]() Quick path
Quick path
Use this page when you need deeper evidence.
Diagnosis
Diagnosis is useful because it gives shared language, but it is never just a label. Clinicians consider distress, impairment, culture, context, and possible rule-outs.
Uncommon behavior is not automatically a disorder.
The same behavior can mean different things across cultures.
Clinicians ask whether symptoms disrupt daily life.
The DSM helps professionals describe symptoms and plan treatment.
DSM categories shift as science, ethics, and culture develop.
One person can meet criteria for more than one disorder.
Note
The same behavior can mean different things depending on distress, time, impairment, culture, and rule-outs.
OCD
OCD involves obsessions, compulsions, or both. The key issue is distress and interference, not neatness.
Obsessions are intrusive and unwanted thoughts, fears, urges, images, or doubts. Compulsions are repeated behaviors or mental acts used to reduce distress, prevent feared outcomes, or feel certain.
Criteria
A simplified DSM-style summary asks whether symptoms are present, whether they cause distress or impairment, and whether another explanation fits better.
Intrusive unwanted thoughts and/or repeated behaviors or mental acts.
Symptoms take significant time or cause distress or impairment.
Symptoms are not better explained by substances or medical conditions.
Clinicians check whether another disorder better explains the symptoms.
Some people doubt their fears; others feel almost convinced.
DSM-5 includes a current or past tic-disorder specifier.

Note
They help separate symptoms, impact, and alternative explanations instead of reducing diagnosis to one visible habit.
DSM changes
OCD moved from Anxiety Disorders into Obsessive-Compulsive and Related Disorders, showing that diagnosis changes as science, culture, and ethics develop.
OCD sat under Anxiety Disorders.
01
It moved to a related-disorders chapter.
02
DSM-5 used “intrusive and unwanted.”
03
Current criteria continue to include insight and tic-related specifiers.
04
Prevalence
Prevalence estimates vary by method, population, and timeframe. These figures give U.S. and global context.
U.S. adult estimates
1.2%
of adults
Past-year U.S. adult estimate.
2.3%
of adults
Lifetime U.S. adult estimate.
Among past-year cases
Among past-year U.S. adult cases.
Worldwide context
1-3%
Estimated worldwide range.
U.S. and global estimates can differ because studies use different diagnostic interviews, timeframes, populations, and because stigma or access to care can affect reporting and diagnosis.
Causes
There is no single cause. OCD is better understood as multiple biological, cognitive, learning, stress, and social factors interacting.
Genetics and brain circuits may play a role.
Stress and trauma may be associated with higher risk, but OCD does not have one single cause.
Uncertainty and threat can feel hard to tolerate.
Rituals can persist when they briefly reduce anxiety.
Stigma can delay help.
Treatment
OCD is treatable. Main approaches include ERP, medication, combined care, and specialized options for severe treatment-resistant cases.
ERP
First-line psychotherapy
Face triggers while resisting compulsions.
8-12 wk
SSRIs / clomipramine
SSRIs are common; response can take weeks.
≈70%
ERP, medication, or both
About 70% of people with OCD respond to ERP, medication, or a combination.
TMS
Not first line
Severe cases may need specialist care.
Note
ERP and related care aim to help people face uncertainty while reducing ritual use over time.
Lived experience
Lived experience shows what symptom lists cannot: OCD can be hidden, stigmatized, and deeply disruptive even when someone appears successful.
Watch the story
Hearing the interview makes the section feel less abstract: symptoms become daily experiences, stigma becomes social pressure, and recovery becomes something people practice over time.
Open on YouTubeContent creator and mental health advocate
“I couldn't blink, walk, or look at something without performing compulsions.”
Her story shows OCD attaching to ordinary actions.
Intrusions, avoidance, and intensive treatment.
Made of Millions articleNeuroscience researcher and OCD advocate
“OCD is not a quirk or choice or adjective.”“It’s immense. It isolates people.”
Her story shows private suffering behind achievement.
Fear, shame, reassurance seeking, and ERP.
NIMH: My Life With OCDKalista: OCD is not just cleaning. Uma: OCD is not a casual adjective.
Kalista: Compulsions affected ordinary actions. Uma: Success hid private distress.
Kalista: Advocacy makes symptoms less hidden. Uma: OCD jokes hide seriousness.
Kalista: Her account emphasizes treatment and advocacy. Uma: Her account emphasizes ERP and hope.
Note
Both accounts show that OCD can be intense, hidden, treatable, and more complex than stereotypes suggest.
Course connection
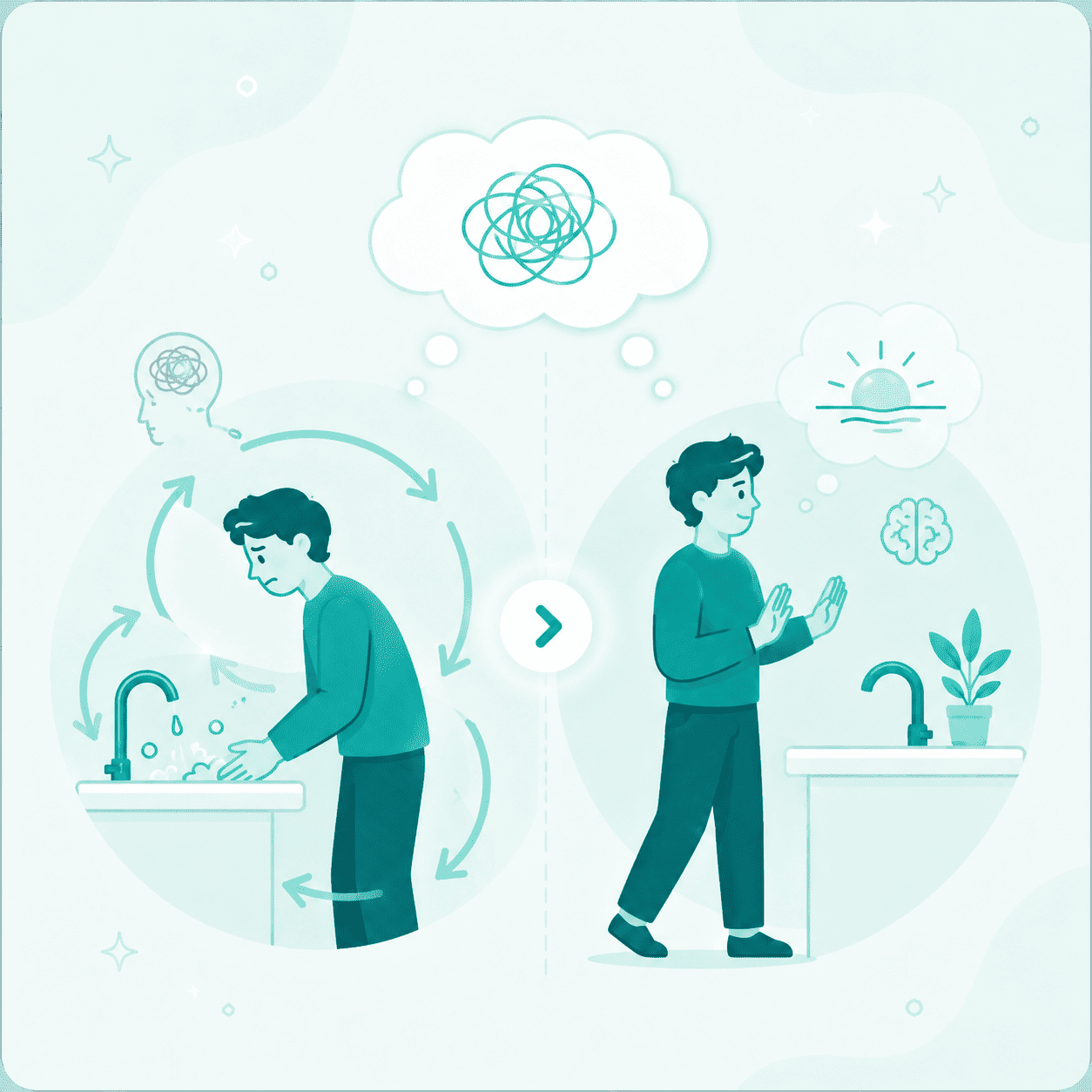
The OCD cycle connects directly to learning theory: a behavior can become stronger when it removes an unpleasant feeling.
Learning through consequences. Negative reinforcement happens when a behavior becomes more likely because it removes something unpleasant. In OCD, a compulsion may temporarily remove anxiety, so the ritual becomes more likely next time.
Compulsions may remove anxiety for a moment, which can make the ritual more likely next time.
Exposure and response prevention practices uncertainty while resisting the ritual.
This is an educational model, not personal medical advice.
Note
This visual belongs here because the section explains why relief can reinforce rituals.
Cycle
Trigger → intrusive thought → anxiety/doubt → compulsion → temporary relief → stronger cycle
The tutorial version lets students test this with a choice: repeat the ritual for quick relief or practice an ERP response.
Sources
Full citations and links used for the project.
This website is for an educational psychology project and is not medical advice.